Too often, trans people’s lives disappear into a morass of medical and legal arguments. Too often, we fail to see the person behind the arguments; the lives behind the debate.
I am writing an academic article about narratability, about the capacity to tell one’s story, and the relationship between that and human rights; the accessibility and reality of rights for trans people. I have returned to this post again and again. It remains difficult to write.
Here is the issue: there is a large lobby of people in this country who wish trans people did not exist. There is a large lobby of people in this country who would rather children were suicidal than that they were trans, or that they were helped. These people have a platform that we do not. I am writing on this blog; they are writing in the newspapers.
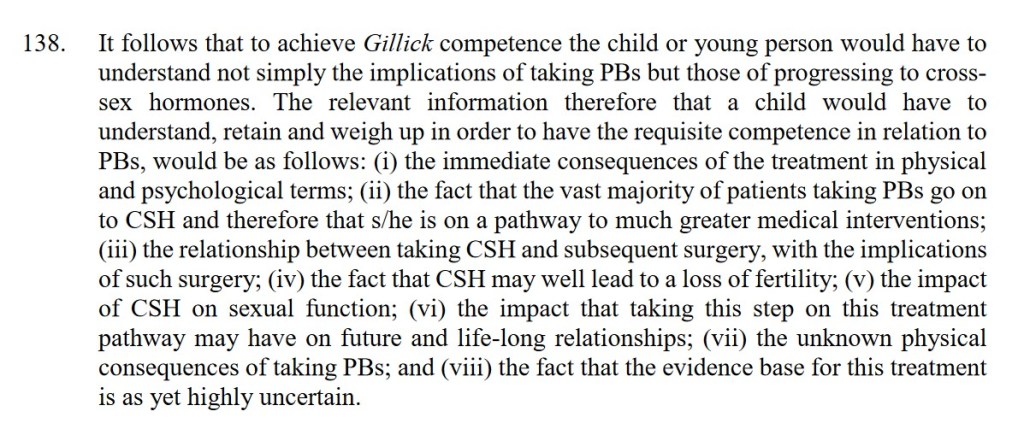
In the past few weeks, the courts here in the UK have decided that children under 16 are very unlikely to be able to consent to puberty blocking hormonal treatment. Puberty blockers are a safe, reversible treatment which are used to delay the onset of pubertal developments which are incongruous with the child’s gender identity. They are recognised worldwide as a useful – indeed, often necessary – intervention for trans children. But the decision of the High Court has meant that it is now highly unlikely that children will be able to access this treatment. It is hard to convey the devastation this is causing for the children affected, and for their families. Overnight, their access to the healthcare that is allowing them to cope with growing up in a world where their interactions with society are shaped by an incongruity between their self-image and society’s perception, has been taken away. Overnight, their safety-net has been ripped from underneath them.
I don’t intend, in this post, to go into the academic or legal aspects of the judgment. I’ve already done that in another post. I want to highlight the human.
Here’s the thing. Trans people should have the right to their stories. Their own stories, of their own lives, lived how they choose. But the restrictions that a cisnormative society – a society that privileges cisgender identity – places them under mean that frequently, they must sacrifice that right in order to be understood by institutions like doctors and courts. The children affected by the Bell ruling have already had to explain themselves over and over to doctors. Now they will have to do the same thing to a judge, before they can access their medications.
Cisnormative institutions understand a particular kind of story. They understand one where trans identity is pathologised – where it is a medical process. They understand the narrative of transition as a definable journey from a point A on a binary scale to a point B on the opposite side. They understand stories where gender identity is fixed and does not fluctuate. We can see this in the terms set out in the Gender Recognition Act 2004 – its insistence that you must choose a gender identity to live in until the end of your life; its requirement of a two-year ‘real life test’ before legal gender recognition can be approved.
But this is not reality. In reality, gender identity is messy and nuanced and fluid, and glorious in its indefinability. People’s identity changes over the course of their life. They identify inside or outside the binary. They transgress gender norms and categories and live in the liminal spaces. Law and medicine do not understand this because of what they are, because they are creatures of rules and norms.
I am writing about how, when applicants came to the European Court of Human Rights to petition for the UK to legislate for legal gender recognition, their stories were taken from this beautiful humanity and distilled down to narratives of surgery, effort, and pain. Before the law would hear them, they had to have gone through medical and surgical interventions. Before they could access those, they had to lay open their lives to doctors. Their transition journeys, as mediated through the lens of medical science, had to be literally written on their bodies in pain before the Court of Human Rights would hear their applications. This does not feel like human rights.
I am struck by the absence of trans people in the reporting around the Bell decision. I am struck by watching three experts in trans and gender law – all trans – defending their lives and experiences to the Women and Equalities Committee of Parliament, and being countered by three non-experts whose qualifications seem to be mainly being academics with opinions.
I want us to do more than hashtag #TransRightsAreHumanRights. They are, of course, and as a human rights lawyer I will defend that to the last. But we seem to be losing the human. I am writing about stories, and I am trying to highlight the loss of stories – because if we do not hear people, really hear them, we cannot possibly hope to share in any constructive actions toward making the world a better place for them to live in.
If society cannot hear who trans people are without making them commit to definitions of gender invented by cisgender doctors; without making them undergo physical transformations so that they conform to cisgender standards of bodily presentation; without having them explain their lives to cisgender judges to gain approval under cisnormative laws; then society as a whole is failing them.
I am writing about stories, and rights, and where they intersect. I am writing for a future where I do not have to do this work. I will listen to the stories that that future will tell.